 Colonoscopy is the gold standard for bowel cancer screening, polyp detection or removal and for investigating digestive symptoms. We are lucky to enjoy a very high standard of colonoscopy in many endoscopy centres in New Zealand and we have some fantastic endoscopists. However, some endoscopists need to “up” their game and even the best endoscopists would welcome anything that makes their practice safer, more effective and successful. As with many aspects of the world around us, Artificial Intelligence (AI) is making its way into our lives, and the world of colonoscopy is no different. AI-based systems, powered by deep learning and convolutional neural networks (CNNs), offer a promising solution to enhance our diagnostic accuracy and reduce our human error during colonoscopy. It’s a brave new world, one that might leave some people a bit worried about AI in healthcare. This article explores this interesting and emerging technology that you might see in use during your colonoscopy procedure.
Colonoscopy is the gold standard for bowel cancer screening, polyp detection or removal and for investigating digestive symptoms. We are lucky to enjoy a very high standard of colonoscopy in many endoscopy centres in New Zealand and we have some fantastic endoscopists. However, some endoscopists need to “up” their game and even the best endoscopists would welcome anything that makes their practice safer, more effective and successful. As with many aspects of the world around us, Artificial Intelligence (AI) is making its way into our lives, and the world of colonoscopy is no different. AI-based systems, powered by deep learning and convolutional neural networks (CNNs), offer a promising solution to enhance our diagnostic accuracy and reduce our human error during colonoscopy. It’s a brave new world, one that might leave some people a bit worried about AI in healthcare. This article explores this interesting and emerging technology that you might see in use during your colonoscopy procedure.
So what’s it all about?
A doctor carrying out a colonoscopy is always vigilant for anything that looks abnormal. In particular, they search for polyps, the small growths that sometimes grow to become cancers. When these are small or camouflaged or covered in a small amount of residual fluid, they can easily be overlooked. It probably happens more often than we care to admit. Certain polyp types are particularly difficult to spot because they are flatter and very similar to the the surrounding mucous membrane lining the bowel. These are called Sessile Serrated Lesions and they are a bit notorious for evading us and of becoming cancers in a relatively shorter time when compared to conventional polyps.
Imagine that a polyp wasn’t spotted and the patient was given the “all clear” and discharged from further follow-up and you’ll quickly understand the repercussions: some years down the line the polyp presents as a cancer and the patient has to go through major surgery or adjuvant treatments like chemotherapy or radiotherapy. Unfortunately, sometimes the cancer is already too established to cure. CADe systems are designed to identify potential polyps, in real-time, during the colonoscopy. These systems highlight suspicious lesions on the monitor to alert the endoscopist. The endoscopist must then pause to inspect the area more carefully.
One of the key performance indicators (KPIs) in endoscopy is the doctor’s rate of detecting polyps known as adenomas. This Adenoma Detection Rate ought to be over 25% for male patients and over 15% for female patients (women produce fewer polyps than men do). Several studies have demonstrated that CADe improves an endoscopists’ ADRs by up to 14%. Another study showed that significantly higher ADRs were achieved when groups of endoscopists used AI compared to when they didn’t use this technology and simply relied on their eyesight.
In short, it’s a win-win for both the endoscopist and the patient.
How do Artificial Intelligence CADe Systems Work?
CADe relies on a technology called Real-Time Video Analysis. The system is integrated into existing camera systems and the hard drive controlling the image capture and display. The CADe continuously analyses every frame of the colonoscopy video stream. Colonoscopy videos run at between 25 and 80 Frames Per Second! Each frame is inspected for features that might indicate a polyp in the frame: changes in mucosal colour or texture, small elevations or bumps on the surface, the pattern of the “pits” making up the surface (think of paving stones or bricks laid on a driveway). This information is placed into an algorithm created by AI and within a split second the information is cross-referenced with a database of similar data points seen in known polyps. Data from up to 40,000 pictures of known polyps of every shape, size, type, colour, pattern, contour and angle of view is used to make a “match”. Think of an elaborate card game of SNAP! played with 40,000 different playing cards. In a split second the computer places a visual ring around the polyp on the screen, allowing the doctor to pause and re-inspect the questionable area.
The doctor then has the choice of ignoring the area in question or, if they are convinced after a second look at the polyp, they can remove it. The AI can learn from its successes and failures. Many CADe systems use advanced algorithms to filter out artifacts like air bubbles, stool, or folds in the colon. To prevent unnecessary distractions from AI misidentifying abnormalities, the system’s sensitivity can be turned down or up by the endoscopist.
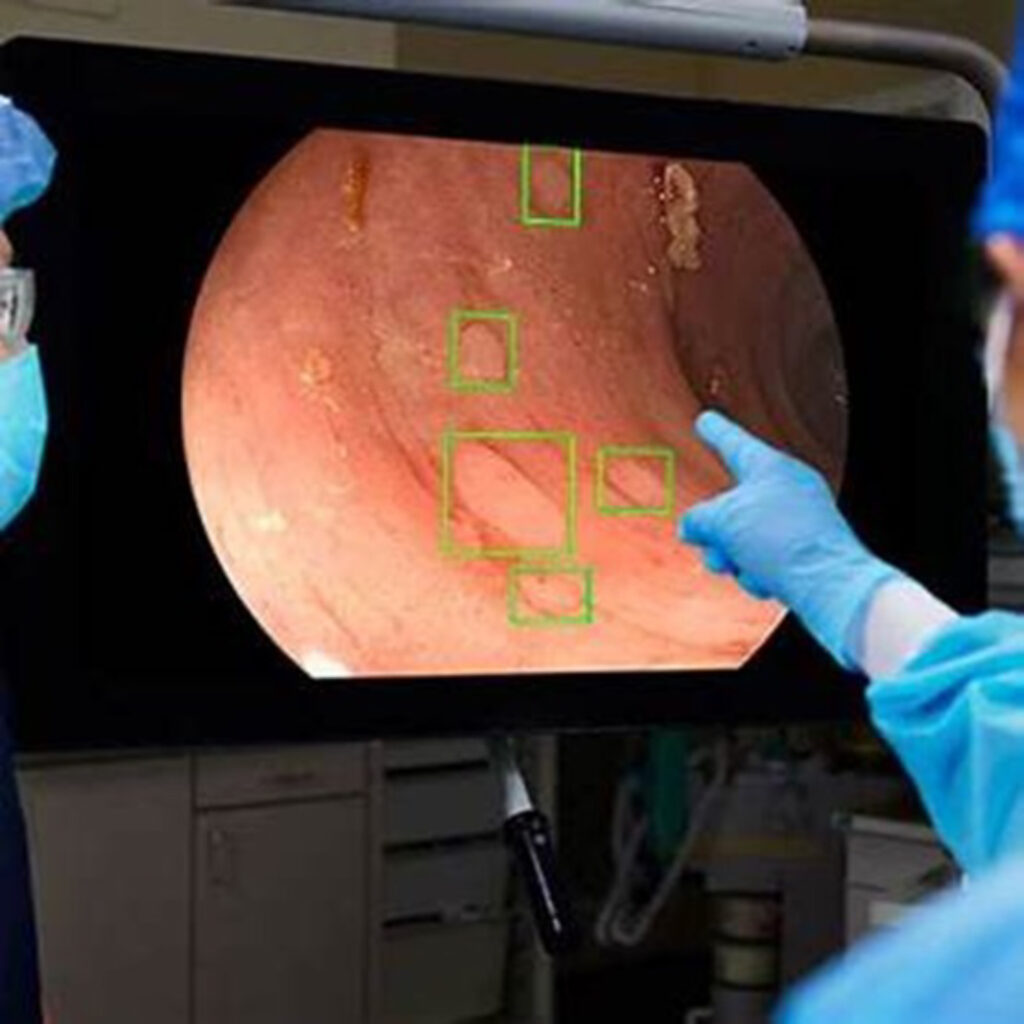
AI highlighting small flat polyps in the bowel
How else is AI being used in colonoscopy?
AI is a burgeoning technology and one aspect that is yet to be brought fully into clinical practice is Computer-Aided Diagnosis (CADx). CADx focuses on polyp characterization—distinguishing between benign hyperplastic polyps that could arguably be left inside you without consequence and the more worrying polyps called adenomas that need to be removed. By analysing surface patterns, colour, and vascular structures, CADx provides a real-time “virtual” histological assessment. This might reduce the need for unnecessary biopsies and removal of polyps. At present CADx has accuracy rates of over 90%, but we cannot rely yet on a system that gets 1 in 10 diagnoses wrong.
AI integration in colonoscopy not only improves ADR but it might also streamline workflows and ensure standardisation of endoscopy practice globally. AI systems can automatically document findings to create a report that does not require manual data input or dictation. It will be able to suggest follow-up intervals based on the best practices guidelines from world authorities, leaving it less to the whim of the endoscopist. AI can link your personal details with pathology specimens sent to the pathology laboratory, sending this information to the pathology lab in advance of the specimen arriving there. This can perhaps reduce your wait for news on the polyps, especially if it can also send the report to you at the same time as the pathologist releases the information to the doctor. At each step in the process, AI can reduce the chance of human error and increase our efficiency. Our biggest challenge with AI at present is the regulation of this technology and the new ethical considerations that AI brings to clinical practice, such as data privacy, algorithm biases and who is liable in case AI makes errors.
In summary, AI is revolutionising colonoscopy by enhancing polyp detection, reducing missed polyps, and aiding in real-time diagnosis. Despite existing challenges, the integration of CADe and CADx systems into clinical practice is becoming increasingly feasible. With ongoing research and technological improvements, AI will likely play a pivotal role in advancing the prevention of bowel cancer and ensure that you receive the best possible treatment. I use Olympus endoscopes for colonoscopy, which have built-in AI for polyp detection. You have nothing to fear from it – I use it merely as an adjunct to careful and patient colonoscopy and to complement my “polyp radar” that has been honed by 25 years of doing colonoscopy. And by the way, I can switch off this AI feature, if you prefer that!
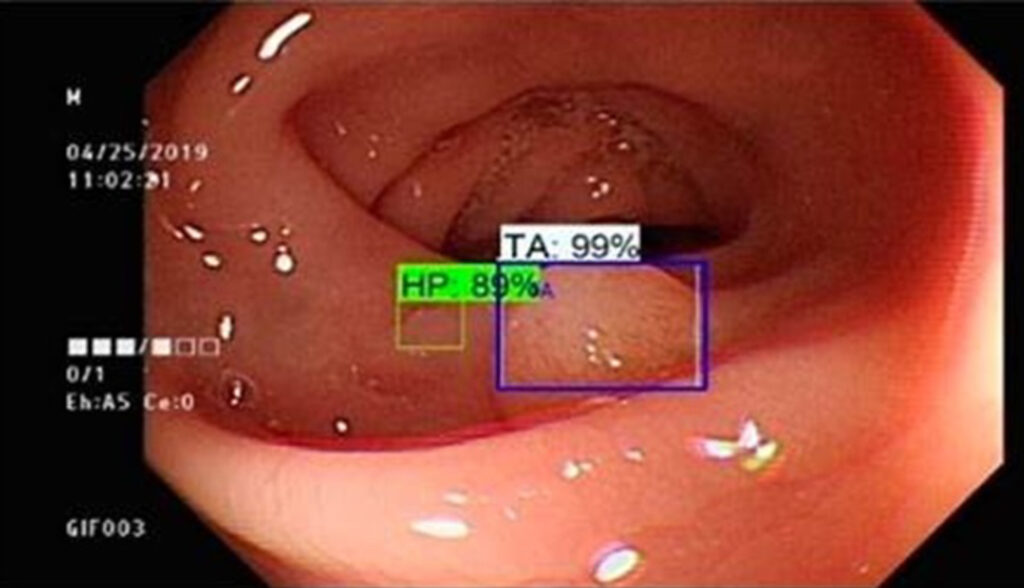
CADx in action, distinguishing a hyperplastic polyp (HP) from a tubular adenoma 9TA)
References
1. Wang, P., et al. “Real-Time Automatic Detection System Increases Adenoma Detection Rate During Colonoscopy.” Gastroenterology, 2020.
2. Mori, Y., et al. “Computer-Aided Diagnosis for Identifying Colorectal Polyps Using Endocytoscopy.” Gastrointestinal Endoscopy, 2019.